Cloud Hospital OS: Security Without On-Premise Complexity
Why cloud-native hospital platforms meet HIPAA, GDPR, and modern privacy law — without the rack, VPN, and patch cycles on-premise demands.
Hospital IT teams are tired of being hardware operators. Rack failures, VPN sprawl, unpatched lab interfaces, and backup drills that never quite prove restore — on-premise was supposed to mean control. Often it means delayed upgrades and six vendors blaming each other after an incident.
What cloud actually changes
- Security patches ship continuously — not when your team finds a maintenance window
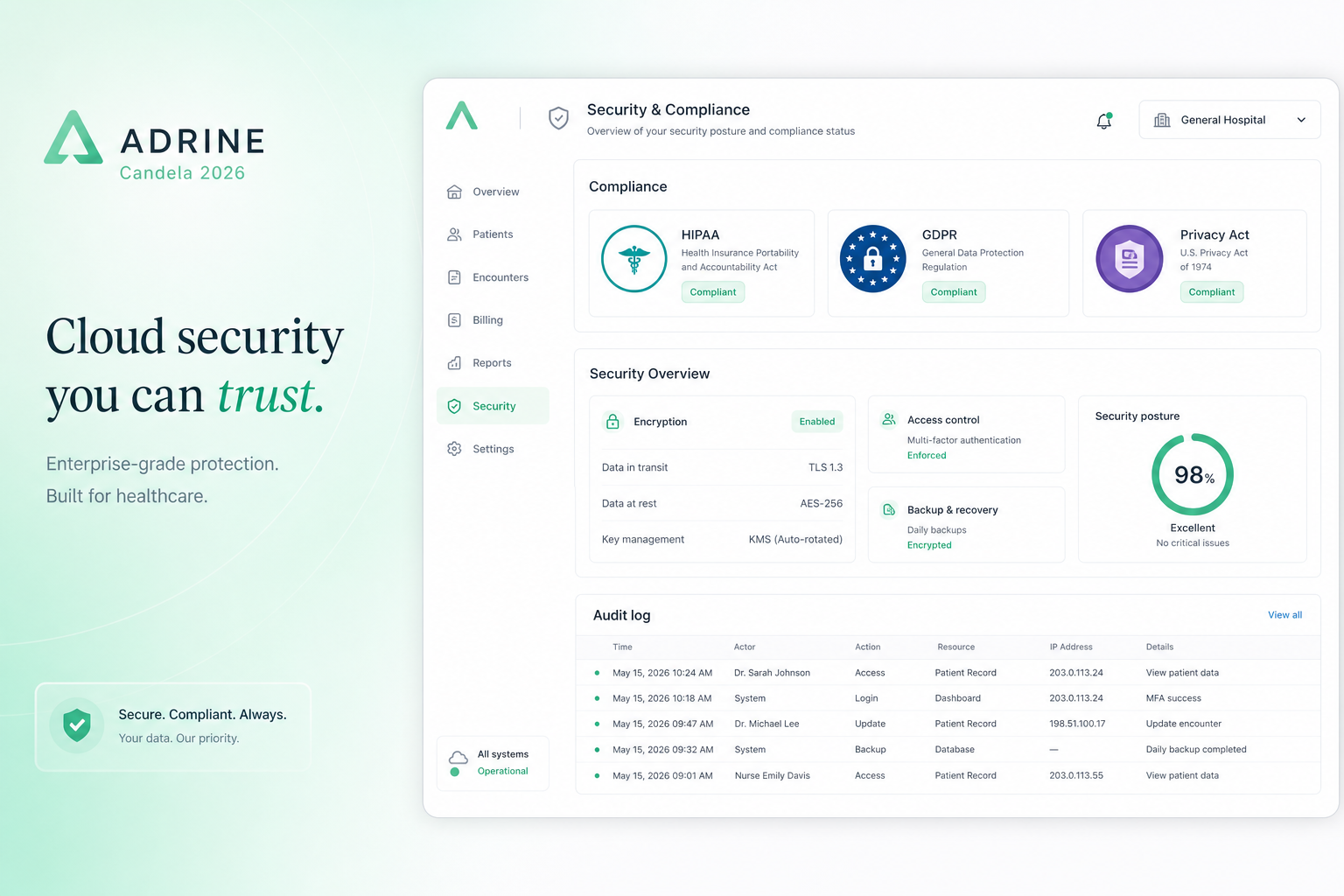
- Encryption at rest and in transit is baseline, not a change request
- Role-based access and session audit trails are product features, not custom projects
- Disaster recovery is replicated infrastructure — not a tape in a basement
- One platform boundary — fewer PHI export points than six integrated systems
US: HIPAA-aligned architecture
US buyers should verify Business Associate Agreement availability, access logging, minimum-necessary role design, and breach notification commitments. A hospital OS reduces shadow IT — the Excel macros and personal WhatsApp groups that HIPAA audits fear as much as servers.
UK and EU: GDPR and operational reality
GDPR is not only legal text — it is access control in daily work. EU and UK hospitals need consent capture, lawful basis documentation, subprocessors transparency, and erasure workflows. Centralizing on one hospital OS beats spreading patient data across disconnected SaaS tools with uneven DPAs.
New Zealand and Australia: Privacy Act and HIPC
NZ providers under the Privacy Act 2020 and Health Information Privacy Code need clear data location, access auditing, and vendor accountability. Cloud hospital OS vendors should document where PHI lives and how cross-border access is blocked or approved.
India: cloud without the on-premise myth
Indian hospitals often assume cloud means data leaves their control. Modern India-hosted cloud meets DISHA expectations with in-region storage, ABHA-ready APIs, and audit trails for NABH — without hospital staff managing servers.
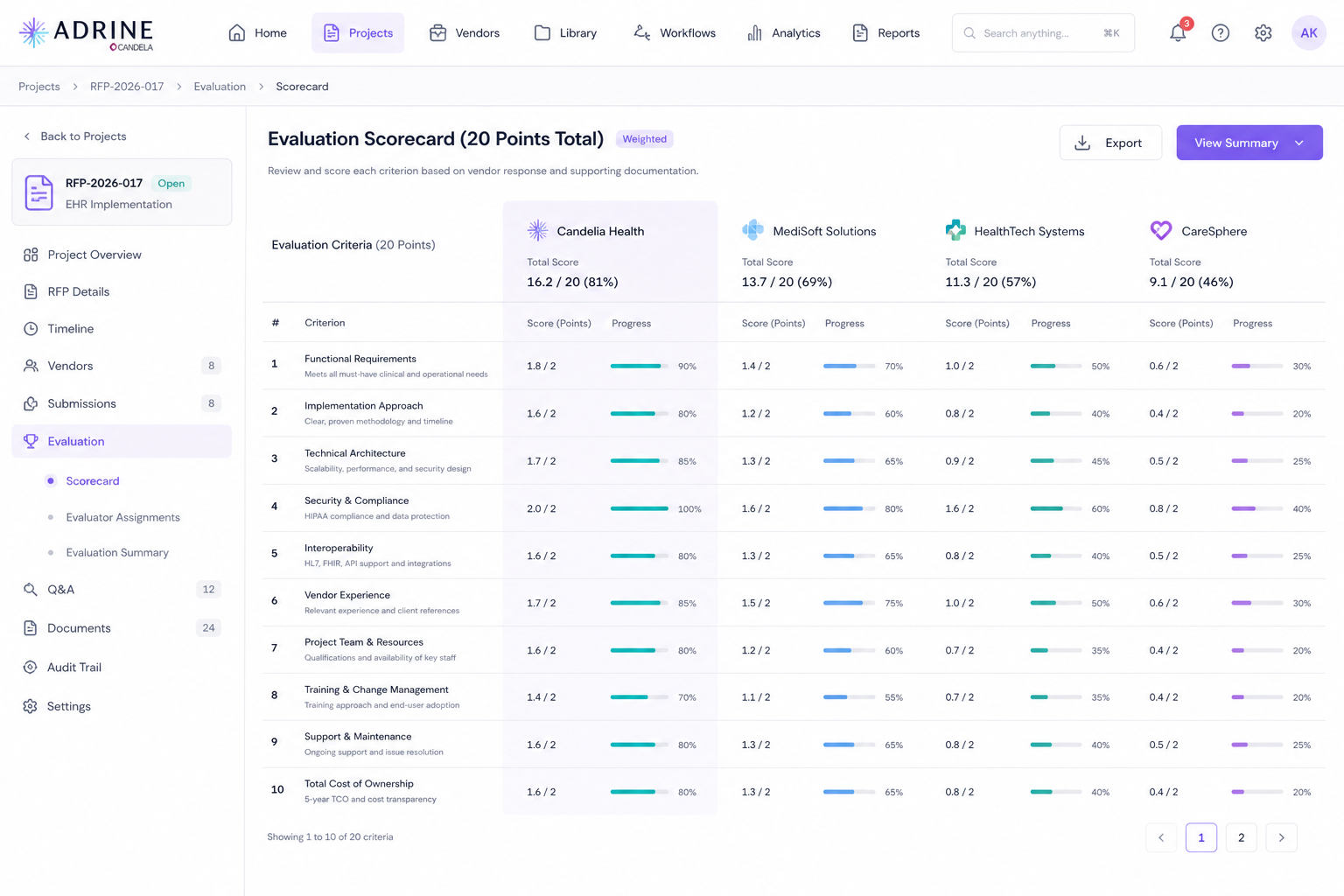
Security questions for your RFP
- Where is PHI stored and which subprocessors touch it?
- How are roles scoped to minimum necessary access by department?
- What audit log retention and export do you provide for accreditation?
- How fast do you patch critical CVEs — hours or quarters?
- What is your measured RPO/RTO for disaster recovery?
The most secure hospital in 2026 is not the one with the most servers on site. It is the one with the fewest places patient data can leak — and the fastest path to prove who accessed what, when.
Frequently asked questions
- Is cloud hospital software HIPAA compliant?
- Cloud hospital software can support HIPAA compliance when the vendor offers encryption at rest and in transit, role-based access, audit logs, BAA availability, and documented incident response. Compliance is a shared responsibility — architecture plus hospital policy.
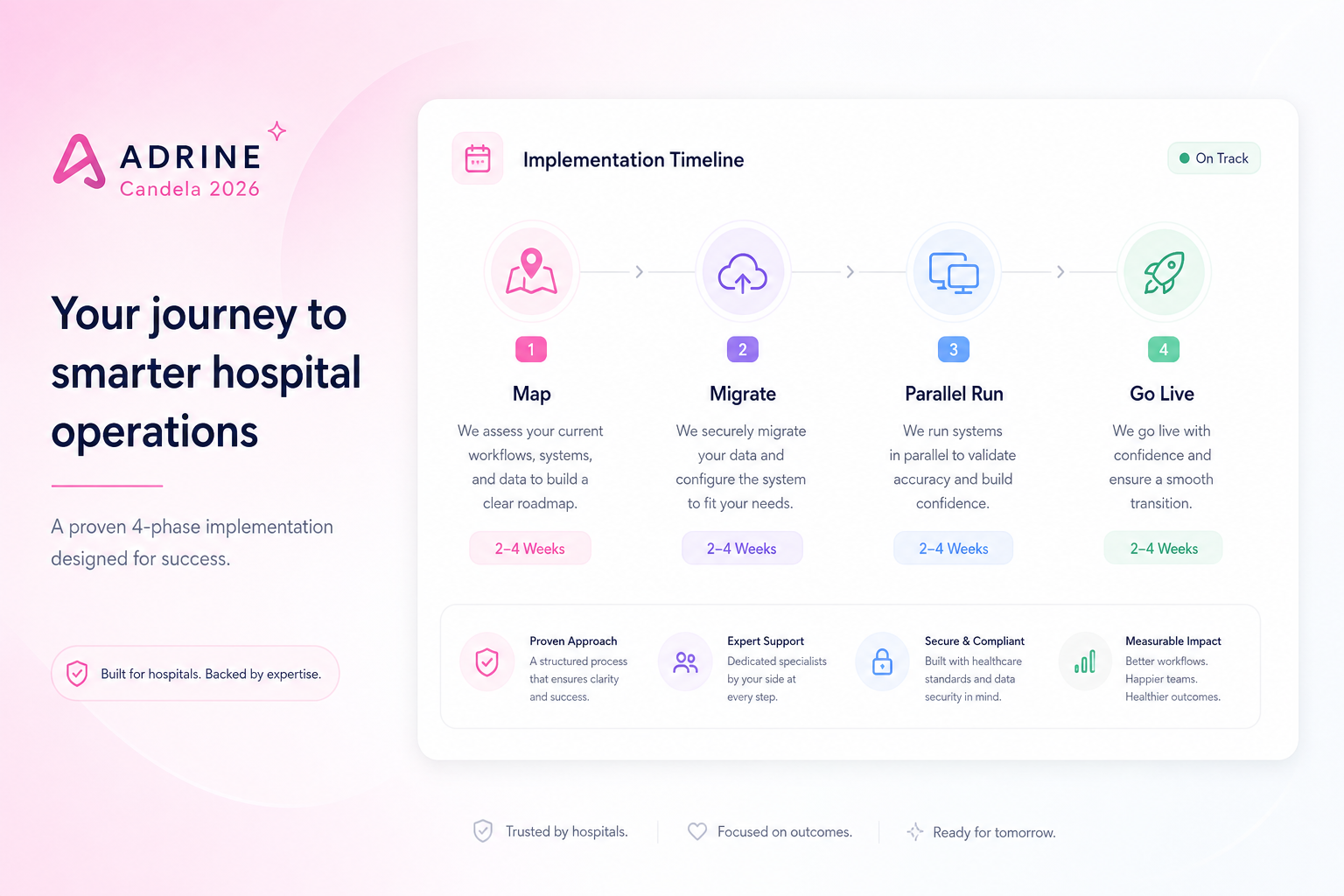
- Why are hospitals moving to cloud HMS?
- Cloud removes on-premise patching, hardware refresh, and disaster-recovery complexity. Unified hospital OS platforms also reduce integration sprawl that creates security gaps between disconnected systems.
- What should EU hospitals verify for GDPR?
- Verify data residency options, DPA terms, subprocessors list, consent workflows, right-to-erasure process, and breach notification SLAs. A hospital OS should centralize access control instead of spreading PHI across six vendors.