Hospital OS Implementation: Go Live in Weeks, Not Years
A phased implementation map — migrate, parallel run, cutover — that works for US, UK, EU, and India hospitals without stopping patient care.
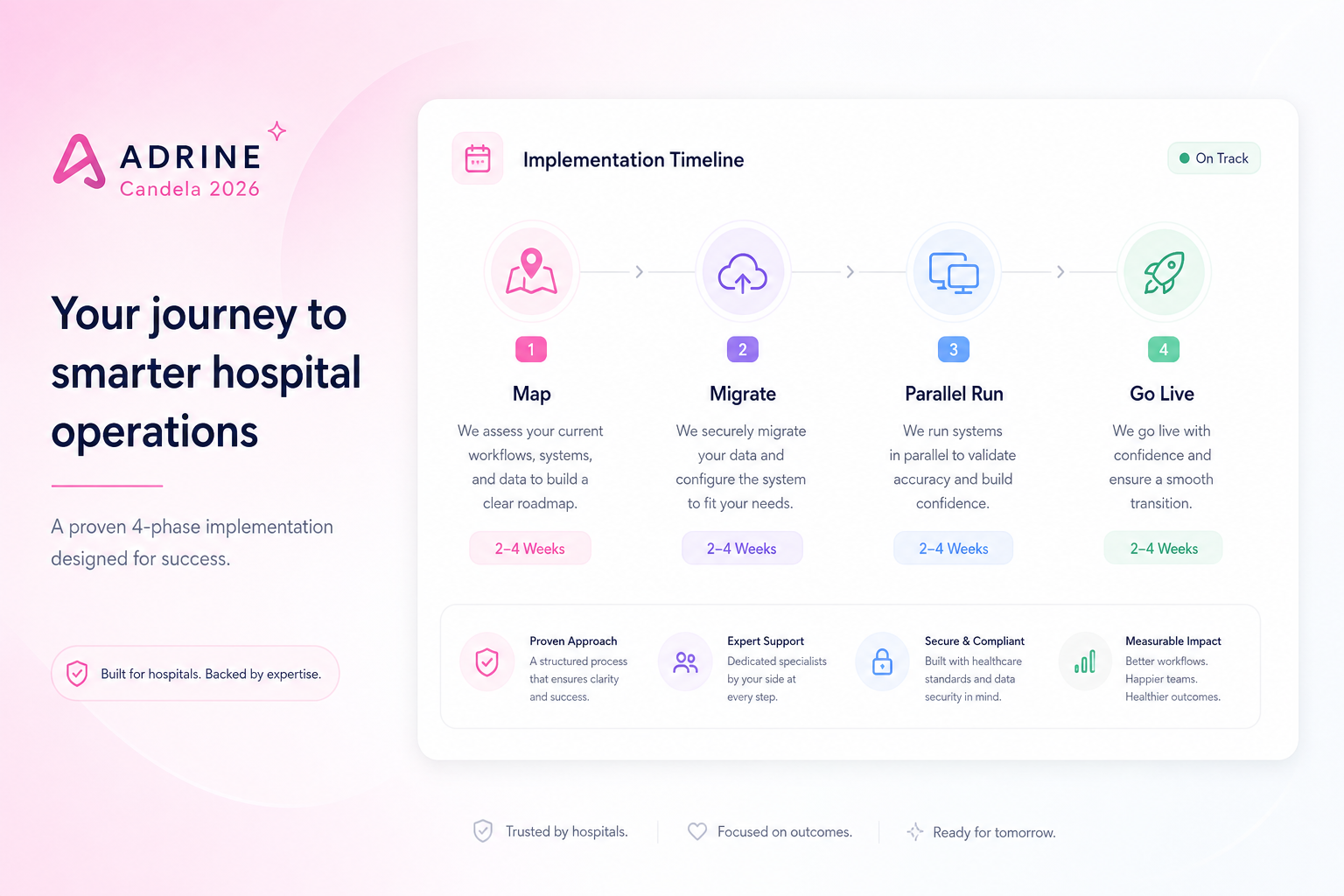
Hospitals do not fail go-live because software is impossible. They fail because vendors sell big-bang cutovers, IT maps every edge case upfront, and wards stop trusting the system on day three. Modern hospital OS implementations work differently: small waves, parallel run, and leadership visibility from wave one.
Phase 1 — Map your hospital (days 1–5)
Document bed count, departments, payer mix, and the six systems you are retiring. Identify the three workflows that touch revenue daily — usually registration, consultation or admission, and billing.finalization. Everything else schedules behind them.
Phase 2 — Configure modules (days 5–12)
- Charge masters, packages, and service tariffs
- User roles aligned to minimum necessary access
- OPD queues, tokens, and doctor schedules
- Ward and bed structure for IPD
- Lab and pharmacy catalogs if wave one includes diagnostics
Phase 3 — Migrate and validate (days 10–15)
Migrate active patients, open encounters, and master data — not twenty years of PDF scans on day one. Validate record counts, open bills, and inventory baselines with finance and nursing sign-off.
Phase 4 — Parallel run (days 15–25)
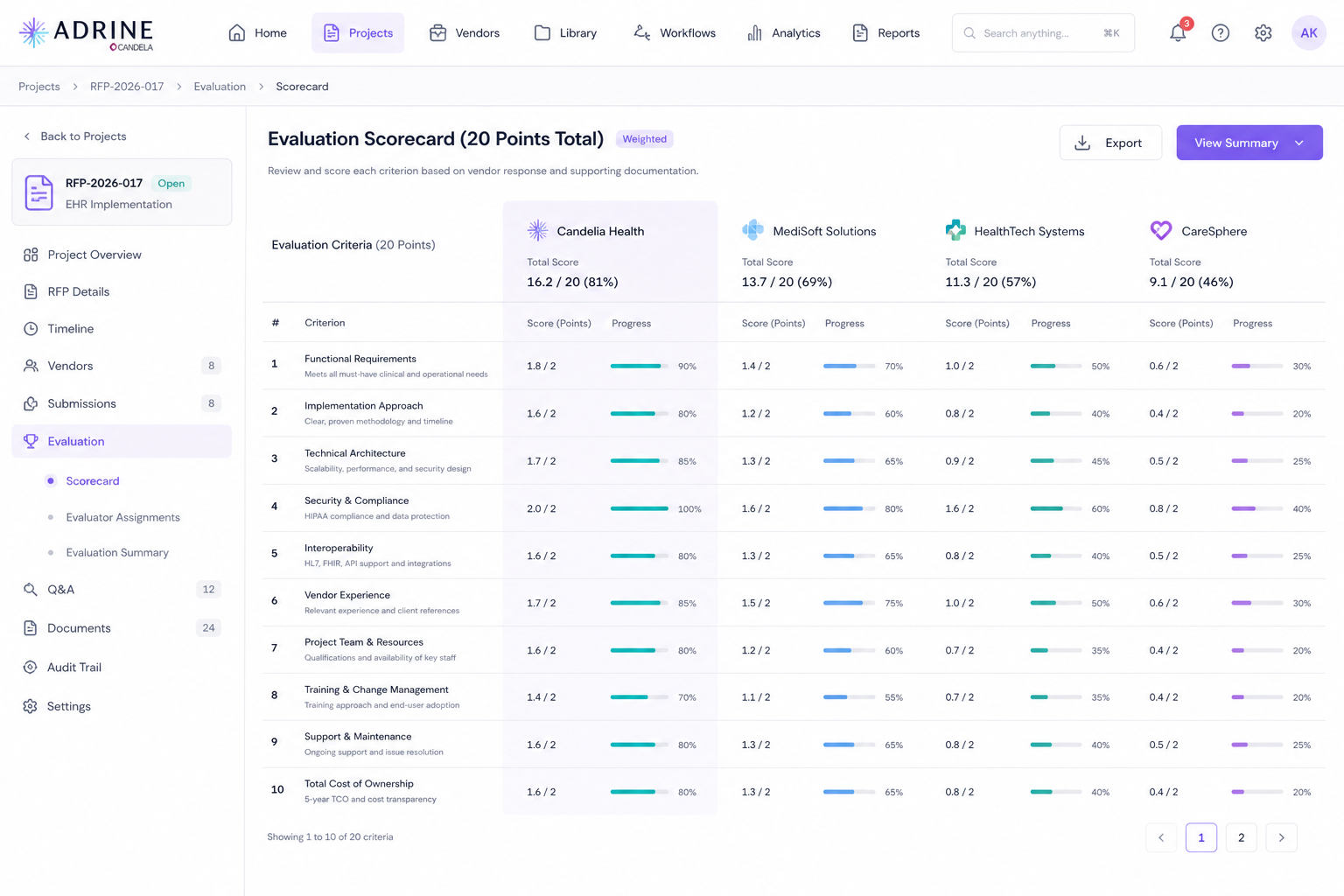
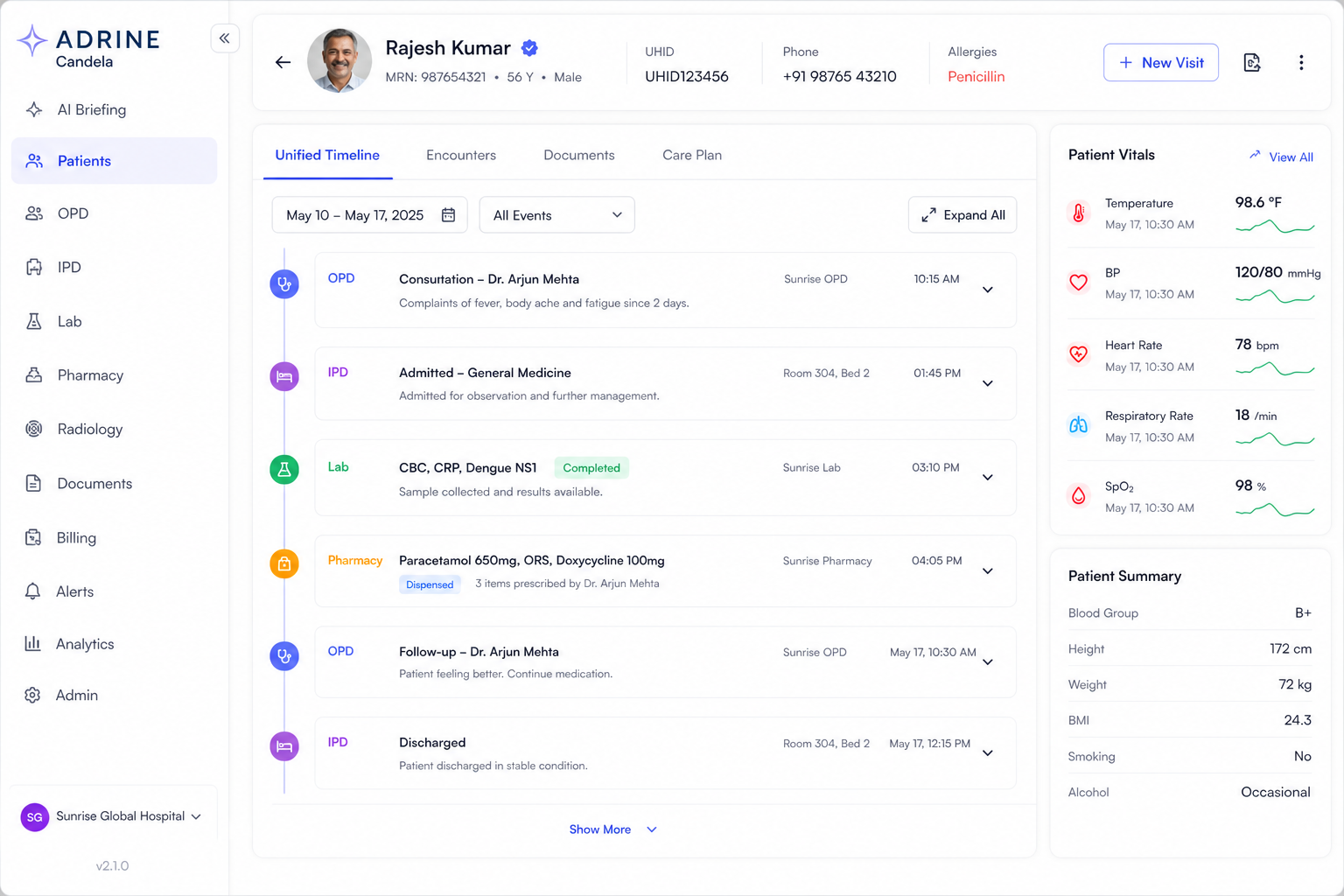
Staff double-enter or shadow-compare critical paths. Finance reconciles daily collections. Nursing confirms orders and results appear in one timeline. Fix gaps before cutover — not after patients notice.
Phase 5 — Cutover and expand
Retire the old system department by department. Turn on command center layers as data quality proves out. US sites add RCM rules; UK sites add pathway metrics; India sites enable ABHA and TPA workflows — on the same OS wave plan.
Roles that make or break timeline
- Hospital champion with authority to decide workflow defaults
- Finance lead who owns charge masters and reconciliation
- Nursing lead who validates ward workflows early
- IT lead who stops scope creep into interface archaeology
Go-live speed is a product decision as much as a project plan. If the platform needs a year of custom interfaces, it is not a hospital OS — it is another integration program. Choose architecture that lets you run the hospital next month, not next fiscal year.
Frequently asked questions
- How long does hospital software implementation take?
- Legacy ERP projects often run 12–24 months. A modern hospital OS with phased modules and parallel run typically goes live in 2–8 weeks for core OPD and billing, then expands department by department.
- What is parallel run in hospital IT?
- Parallel run means staff use the new hospital OS alongside the old system for a defined period — verifying bills, queues, and records match before cutover. It reduces go-live risk without freezing operations.
- Which department should go live first?
- Most hospitals start with registration plus OPD or billing — wherever revenue and patient volume concentrate. Inpatient and lab follow once master data and charge masters are validated.