Unified Patient Record Across OPD, IPD, Lab & Pharmacy
Why one live patient timeline beats interfaces — for outpatient queues, inpatient wards, lab results, and pharmacy dispensing in hospitals worldwide.
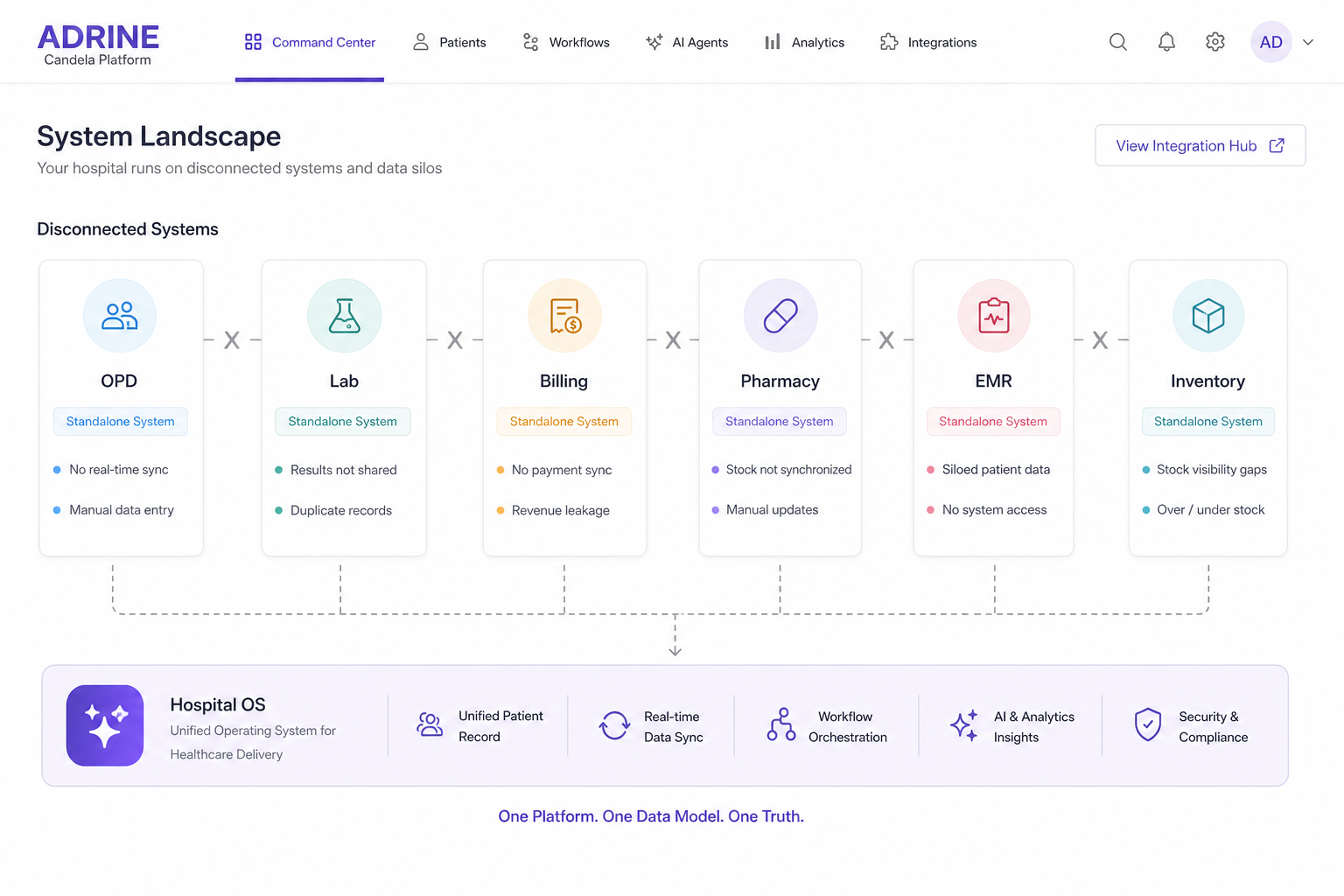
Patients experience one hospital. Software experiences six. Registration knows the name. Lab knows the test ID. Pharmacy knows the formulary code. Billing knows the tariff. Nursing knows the ward. None of them share the same clock — and that is when medication delays, duplicate tests, and lost charges appear.
What belongs on one timeline
- Identity — ABHA in India, MRN everywhere, insurance or NHS number where applicable
- Encounters — OPD visits, admissions, transfers, discharge
- Orders — labs, imaging, procedures, medications
- Results and fulfillment — result values, dispensing, administration
- Charges and authorizations — packages, exclusions, prior auth status
- Documents — consent, summaries, operative notes, discharge instructions
OPD: where the record starts
Outpatient is the highest-volume front door. Queue management, token display, consult notes, and same-day orders must write to the record immediately — not export tonight. US and UK buyers call this patient flow; India calls it OPD. The architecture requirement is identical.
IPD: continuity without re-registration
Admission should extend the same encounter thread — bed assignment, nursing charts, MAR, transfers, and discharge planning. Re-admission as a new identity is how hospitals lose history and duplicate tests.
Lab and pharmacy: close the loop
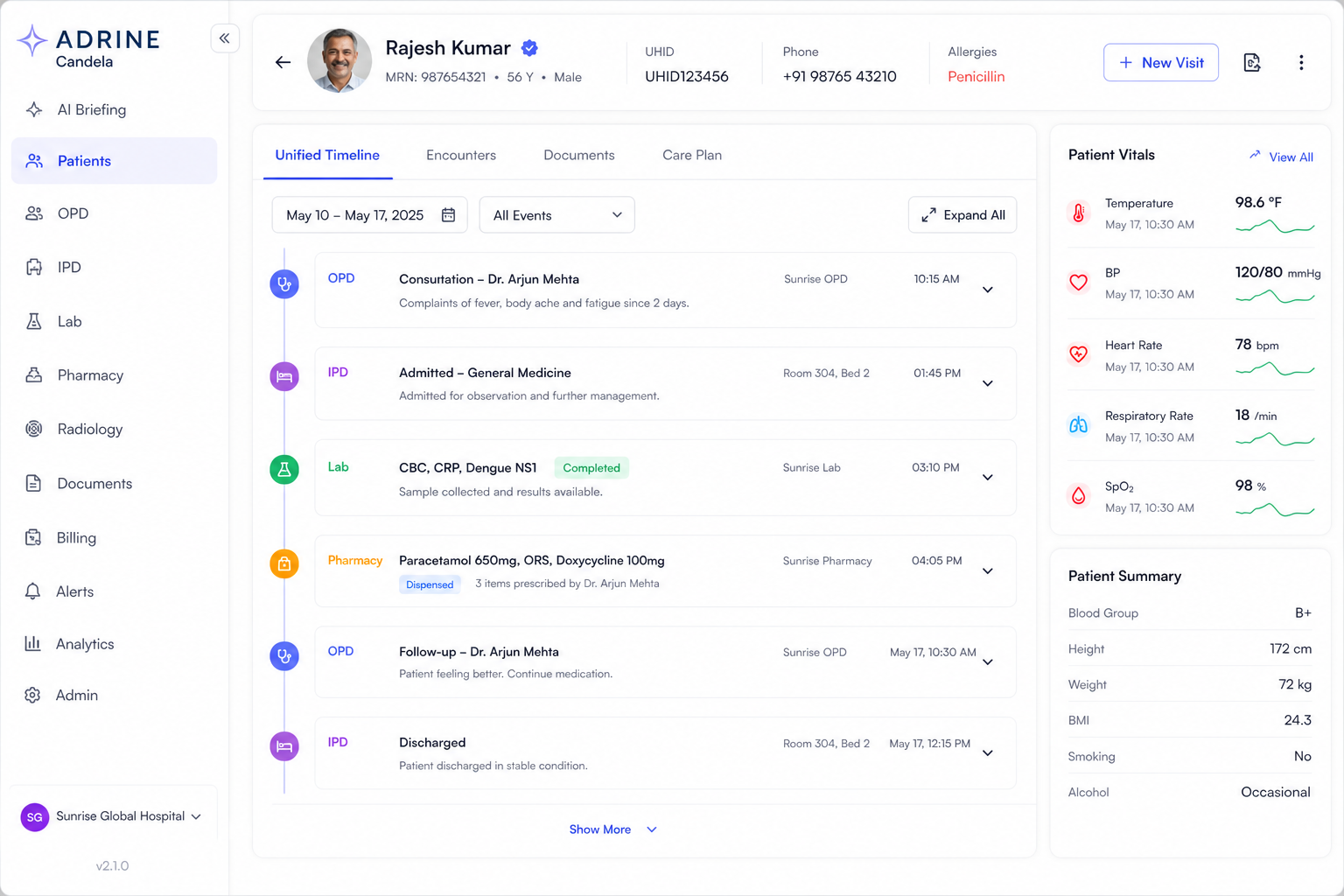
Orders without results in the same UI create callback chains. Results without billing hooks create leakage. Pharmacy dispensing without allergy and interaction context creates risk. A hospital OS closes the loop in one record — order placed, sample collected, result verified, charge captured, medication dispensed.
Regional labels, one architecture
US teams ask for interoperability and EHR integration. UK teams ask for shared care records. EU teams ask for EHDS-ready exchange. Indian teams ask for ABHA linkage. The unified record is the prerequisite — exchange standards matter only after internal truth exists.
Measure unified record quality in one week
- Pick ten random inpatients — how many clicks to see labs, meds, and charges together?
- Time from lab result entry to nursing notification — seconds or hours?
- Count bills with missing line items tied to documented orders
- Ask registrars how often they re-create patients who already exist
Interfaces move copies. A hospital OS preserves truth. Unified patient record is not a feature checkbox — it is the difference between a hospital that runs and a hospital that reconciles.
Frequently asked questions
- What is a unified patient record in a hospital?
- A unified patient record is a single timeline of demographics, encounters, orders, lab results, imaging, medications, charges, and documents — updated in real time across OPD, IPD, emergency, lab, and pharmacy without batch sync.
- How does a unified record help billing?
- When clinical events and charges share one record, fewer items are missed between nursing, lab, pharmacy, and finance. US hospitals see fewer denials from missing documentation; Indian hospitals see faster cashless finalization.
- Is a unified patient record the same as an EHR?
- An EHR is clinical-focused. A unified hospital record includes clinical plus operational and financial events — the full journey from queue token to final bill on one OS.