Why Hospitals Still Run 6 Disconnected Systems (And What It Costs)
Fragmented hospital software leaks revenue, doubles data entry, and blinds leadership. A practical cost model for US, UK, EU, and India hospitals.
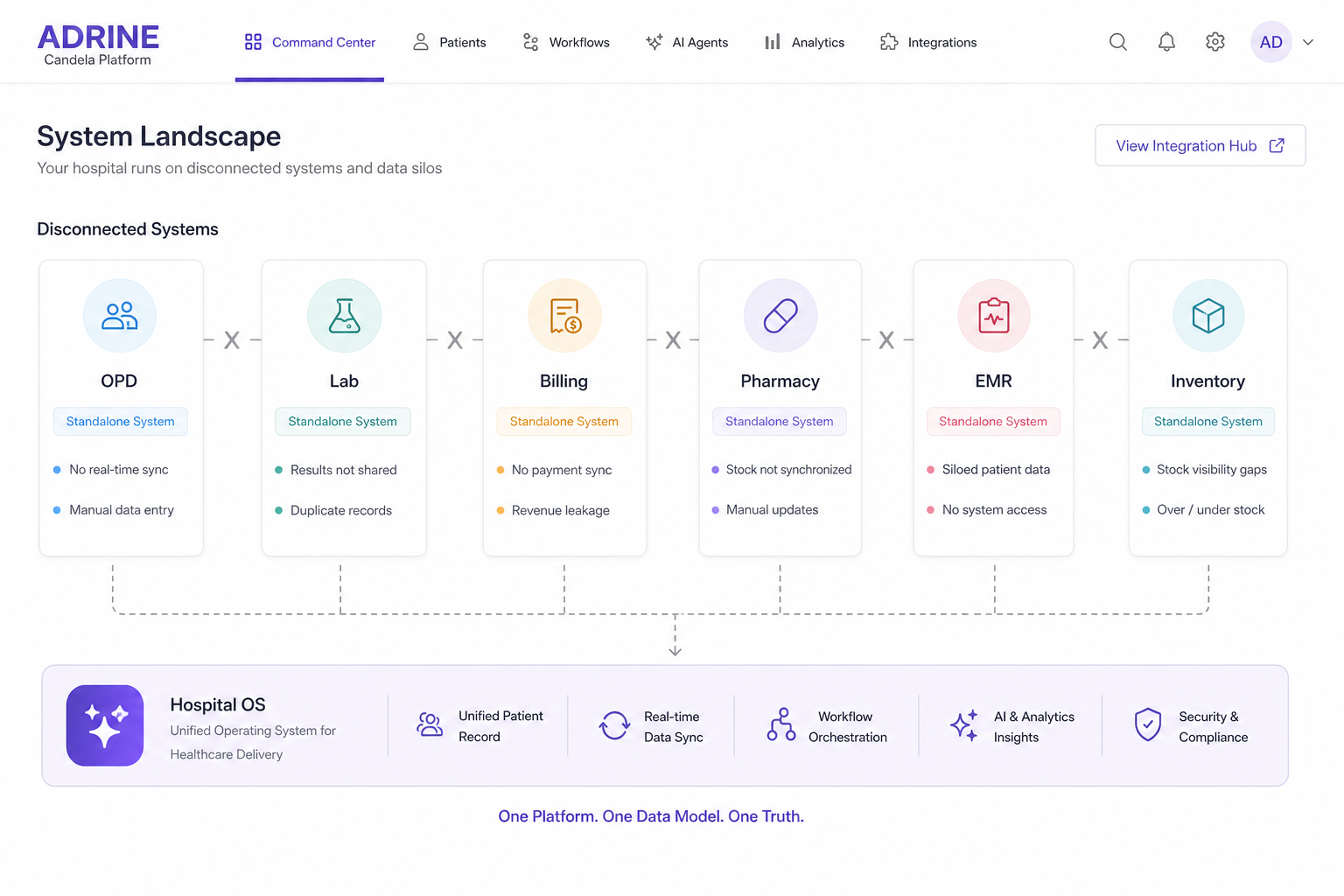
Walk into any mid-size hospital and you will find a familiar archaeology: billing on one platform, lab on another, radiology on a third, nursing notes in a fourth, inventory in Excel, and leadership KPIs in a Monday morning PowerPoint. Each system was a rational purchase. Together they are an irrational operating model.
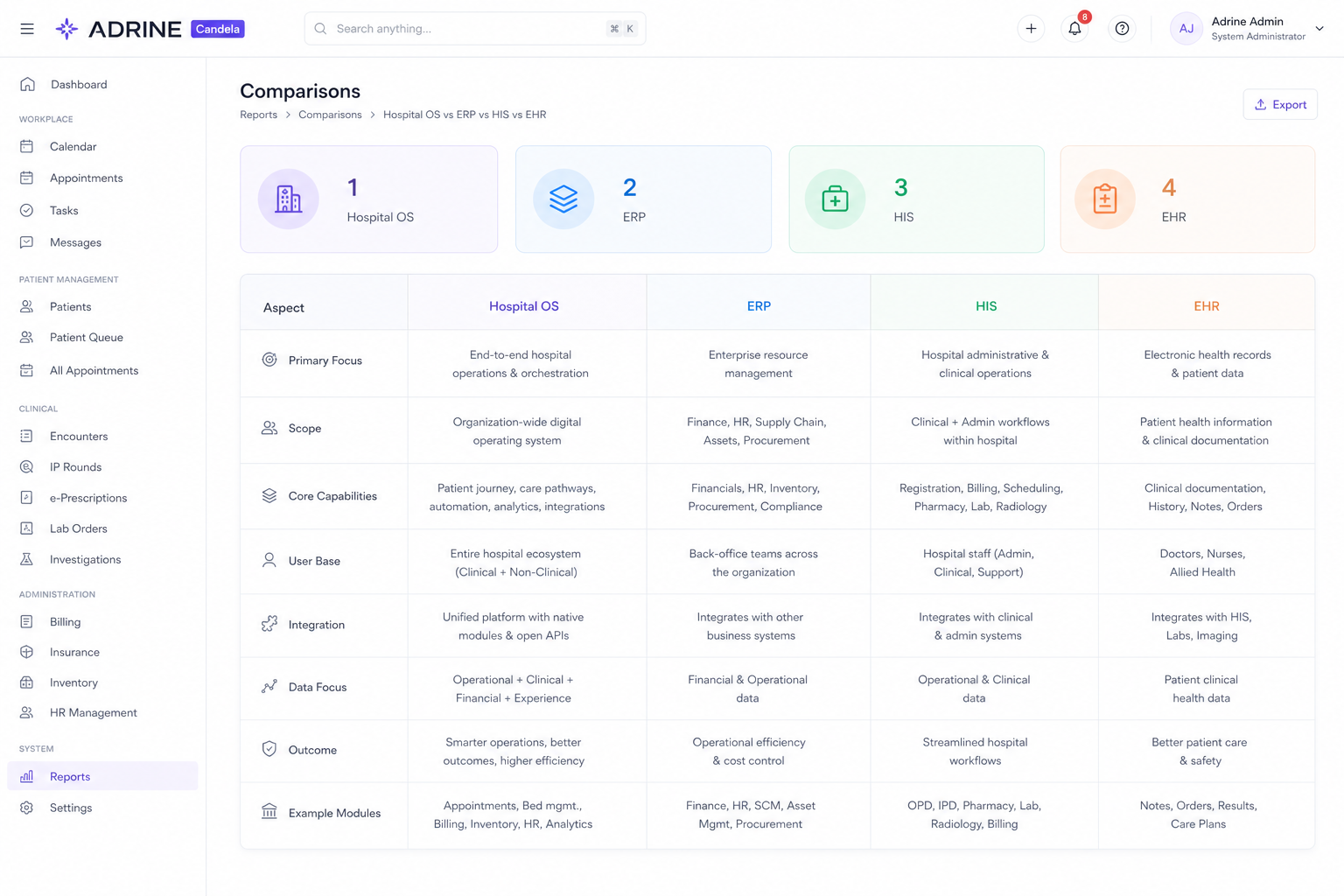
The six-system pattern
- Registration and OPD scheduling
- Inpatient EMR or nursing documentation
- Laboratory information system
- Radiology or PACS
- Pharmacy and inventory
- Billing, RCM, or finance — often partially outside clinical flow
Add WhatsApp for doctor coordination and Google Sheets for bed management and you have a seventh and eighth layer IT does not officially support. This is normal. It is also expensive.
Where the money leaks
Revenue leakage
Charges that never leave the ward because nursing and billing use different timestamps. Package exclusions missed at admission. US denials from prior-auth documentation living outside the clinical record. India cashless claims delayed because discharge summary and bill finalization are on different clocks.
Staff time
Every interface boundary is someone re-typing a patient ID, a test code, or a charge master line. Multiply ten minutes per admission across 800 admissions a month. That is not IT overhead — it is nursing and billing salary spent being middleware.
Leadership blind spots
When bed occupancy lives in one system and collections in another, the COO and CFO argue from different truths. Decisions wait for exports. By the time a queue bottleneck appears in a report, patients have already left.
Why integrations do not finish the job
HL7 messages and FHIR APIs help. They do not give you one workflow. An integration can move a lab result. It cannot tell you that the result, the nursing acknowledgment, and the billable event are three separate failure points unless the platform was designed as one OS.
- Interface projects cost money every year — licenses, monitors, vendor change requests
- Version upgrades break pipes — one vendor upgrades, three others lag
- Real-time command centers cannot be built on batch sync
- AI and predictive layers need unified data — not a data lake patched quarterly
Regional symptoms, same disease
US hospitals feel fragmentation as denials and prior-auth friction. UK hospitals feel it as patient pathway delays and duplicate documentation for CQC evidence. EU hospitals feel it as GDPR consent and record-location sprawl. Indian hospitals feel it as TPA delays and NABH audit scrambles. The architecture cure is the same: one hospital OS replacing the federation.
How to measure your fragmentation tax
- Count how many systems touch a single inpatient admission from registration to final bill
- Measure hours spent re-entering data between departments weekly
- Track denials or write-offs tied to documentation timing, not clinical merit
- Ask how long it takes to get real-time bed position and yesterday's collections — if the answer is 'next week', you are paying the tax
The goal is not one vendor for vanity. The goal is one operating layer so your hospital stops paying middleware salaries and starts collecting revenue it already earned.
Frequently asked questions
- Why do hospitals have so many software systems?
- Departments often digitize independently — billing first, then lab, then pharmacy — each with its own vendor and timeline. Without a hospital OS strategy, integrations accumulate until IT spends more time maintaining pipes than improving care.
- How much does hospital software fragmentation cost?
- Costs include duplicate data entry (hundreds of staff hours monthly), revenue leakage from missed charges and denials, interface maintenance fees, and delayed decisions from stale reports. Mid-size hospitals often lose 2–5% of collectible revenue to operational gaps.
- What is the fix for disconnected hospital systems?
- Consolidate onto a hospital OS with one patient record and retire shadow spreadsheets. Phase by department with parallel run — not a big-bang rip-and-replace of every interface on day one.